
Social and Psychological Influences on Appetite and Eating Behaviors

- Bobby Cheon,
PhD, Stadtman Investigator, Social and Behavioral Sciences Branch, DiPHR - Julia Bittner, PhD, Postdoctoral Fellow
- Yangyang Deng, PhD, Postdoctoral Fellow
- Sarah Baker, BS, Postbaccalaureate Fellow
- Aleah Brown, BS, Postbaccalaureate Fellow
- Nitya Kari, BA, Postbaccalaureate Fellow
- Otiti A. Mayo, BS, Postbaccalaureate Fellow
- Matthew Siroty, BS, Postbaccalaureate Fellow
- Bao-Vi Tran, BA, Postbaccalaureate Fellow
Diet-related disorders such as obesity and type 2 diabetes show pronounced socioeconomic disparities, with higher prevalence among children and adults from socioeconomically disadvantaged households (e.g., lower income or social standing). Socioeconomic disadvantage can limit access to healthier foods and lifestyles and may also shape psychological processes that influence food preferences, eating behaviors, and appetite regulation. Our work aims to identify psychological mechanisms that contribute to the development of these diet-related health disparities. We examine how social factors, including experiences of socioeconomic disadvantage, shape food preferences, eating behaviors, and appetite regulation across development. Using a combination of experimental studies, observational research conducted at the NIH Clinical Center, and population-level approaches, we investigate how these vulnerabilities influence food-related behaviors and health outcomes. Through this work, we seek to (1) identify social factors that promote obesogenic eating behaviors, (2) improve prediction of which children are at greater risk (or show resilience) to developing obesity and cardiometabolic disorders later in life, and (3) inform interventions aimed at reducing socioeconomic disparities in these conditions.
The role of subjective social status on appetite and eating behaviors of children and adolescents
Subjective social status (SSS), i.e., individuals’ perceptions of their position within the social hierarchy, is a major psychosocial determinant of health behaviors and outcomes, independent of objective socioeconomic indicators such as income. Lower SSS has been linked to poorer dietary patterns and increased obesity risk. Prior work from our team shows that, among young adults, lower SSS is associated with higher energy intake, selection of larger portion sizes, and greater preference for energy-dense foods [Reference 2]. Children and adolescents may be particularly sensitive to subjective social status because of heightened exposure to social stressors such as teasing and social exclusion, ongoing social identity development, and frequent peer comparisons in school settings. Despite this vulnerability, the role of SSS in shaping eating behaviors and adiposity during youth remains understudied.
Using data from the NICHD Children’s Growth and Behavior Study (NCT02390765), we examined how subjective social status and distress from teasing relate to BMI (body mass index) z-scores, adiposity (fat mass index), and eating in the absence of hunger among youths aged 8–17 years. Teasing-related distress was associated with higher BMI z-scores, greater adiposity, and increased eating in response to negative affect. Although SSS alone was not directly associated with these outcomes, SSS’s relationship with these outcomes was moderated by the effects of teasing distress; lower SSS was associated with greater adiposity and overeating only among youths who reported distress from teasing (Figure 1) [Reference 5]. These findings suggest that the impact of lower perceived social standing on obesity-related outcomes may be amplified by social threats common in childhood and adolescence.
Figure 1. Lower subjective social status is associated with greater adiposity and eating in the absence of hunger among children experiencing teasing distress.
Interactions of subjective social status (SSS) and teasing distress on: A) fat-mass index (n = 114) and B) child-reported eating in the absence of hunger (EAH-C) resulting from negative affect (n = 100). Lower SSS is associated with higher fat-mass index and EAH-C resulting from negative affect only when children reported experiencing teasing distress. *p < 0.05.
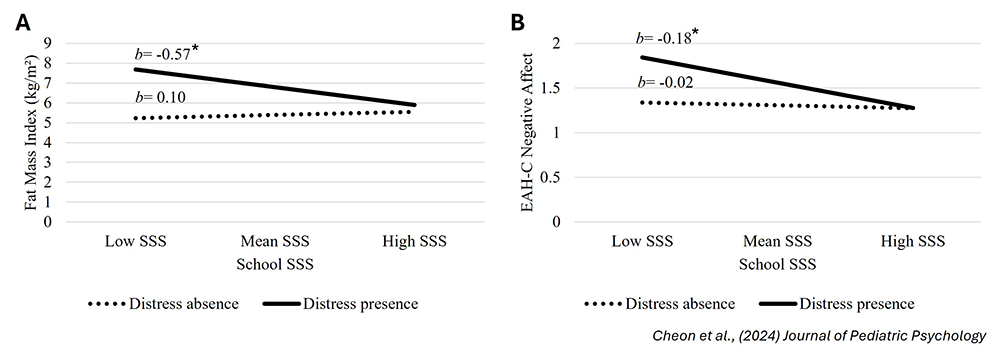
Figure 1. Lower subjective social status is associated with greater adiposity and eating in the absence of hunger among children experiencing teasing distress.
Interactions of subjective social status (SSS) and teasing distress on: A) fat-mass index (n = 114) and B) child-reported eating in the absence of hunger (EAH-C) resulting from negative affect (n = 100). Lower SSS is associated with higher fat-mass index and EAH-C resulting from negative affect only when children reported experiencing teasing distress. *p < 0.05.
We further investigated potential mechanisms linking lower SSS to increased energy intake by testing whether SSS is associated with impaired appetite regulation. In a laboratory paradigm, youths consumed a standardized breakfast shake providing 20% of daily energy needs while fasted. Lower SSS was associated with reduced satiation immediately after shake consumption and greater hunger across the subsequent 90-minute period [Reference 3]. These results indicate that lower perceived social status may blunt satiety signaling in youth, promoting sustained hunger and greater readiness to eat. Early disruptions in appetite regulation may therefore represent a key pathway linking disadvantaged social standing with excess energy intake and elevated obesity risk across development.
Contributions of socioeconomic mobility to dietary patterns and metabolic health
Although lower childhood and adulthood socioeconomic status (SES) has been linked to poorer diet quality, obesity, and metabolic syndrome, it remains unclear whether the trajectory of socioeconomic status one experiences from childhood into adulthood (socioeconomic mobility) contributes to these outcomes. Socioeconomic mobility may impact adult health through changes in financial resources available to engage in healthier lifestyles and psychological strain related to changing status. One under-studied pathway potentially linking socioeconomic mobility to health is through changes in an individual’s perceptions of their SES compared with others (subjective SES).
Using data from the National Longitudinal Study of Adolescent to Adult Health (Add Health), we investigated whether subjective SES contributes to associations of socioeconomic mobility with metabolic health (BMI, metabolic syndrome) and unhealthy diets (high fast-food and sugar-sweetened beverage consumption). We found that participants who experienced substantial upward mobility between adolescence and mid-adulthood had lower risk of high sugar-sweetened beverage consumption compared with those who had consistently low SES from adolescence to adulthood. Additionally, higher subjective SES mediated associations between upward (but not downward) mobility and lower risks of metabolic syndrome, of high fast food consumption, and of high sugar-sweetened beverage consumption [Reference 4]. Overall, upward mobility was associated with higher subjective SES and lower risks of poor metabolic and dietary outcomes. Our findings suggest that while upward mobility may provide more financial and material resources to support better diets and metabolic health, psychological experiences linked to upward mobility also play a unique role in this process and could be a target of future interventions to reduce disparities in metabolic health.
Concerns about maintaining satiety as a driver of opportunistic eating in the context of food insecurity
Approximately 18% of U.S. households with children experience food insecurity, which in high-income countries such as the United States is paradoxically associated with higher obesity risk, particularly among women. One proposed pathway is opportunistic eating, i.e., the tendency to eat in the absence of hunger or to overeat when food is available. Food insecurity during adolescence predicts binge eating and obesity in adulthood, and these behaviors often persist even after food access improves, suggesting that mechanisms beyond food availability are involved.
We propose that enduring anxieties about maintaining fullness or avoiding hunger drive these patterns of opportunistic eating following food insecurity. To test this, we developed a novel construct of satiety insecurity, defined as worry about sustaining adequate fullness independent of current food access. Across six studies in three countries, we assessed satiety insecurity alongside standard food insecurity measures and a virtual portion-size selection task. An individual participant data meta-analysis showed that satiety insecurity mediated the association between food insecurity and preference for larger portion sizes across foods. We further observed serial mediation: higher food insecurity predicted greater satiety insecurity, which predicted larger portion sizes and, in turn, higher BMI (Figure 2) [Reference 1]. These findings suggest that food insecurity may promote opportunistic eating and weight gain by amplifying concerns about insufficient fullness. Ongoing work examines whether satiety insecurity also explains links between childhood food insecurity and other opportunistic eating behaviors beyond portion size.
Figure 2. Serial mediation depicting indirect effects of satiety insecurity and portion selection on the relationship between food insecurity and BMI
Food insecurity is associated with higher satiety insecurity, which is associated with selection of larger virtual food portion sizes, which is in turn associated with higher BMI. The coefficients for the paths (a, b, c’, and d) and the total and indirect effects are based on aggregating individual participant data across six studies into an individual participant database meta-analysis (total n = 1,240). Coefficients are un-standardized and pooled across 25 multiply imputed datasets. Parentheses indicate 95% confidence intervals.
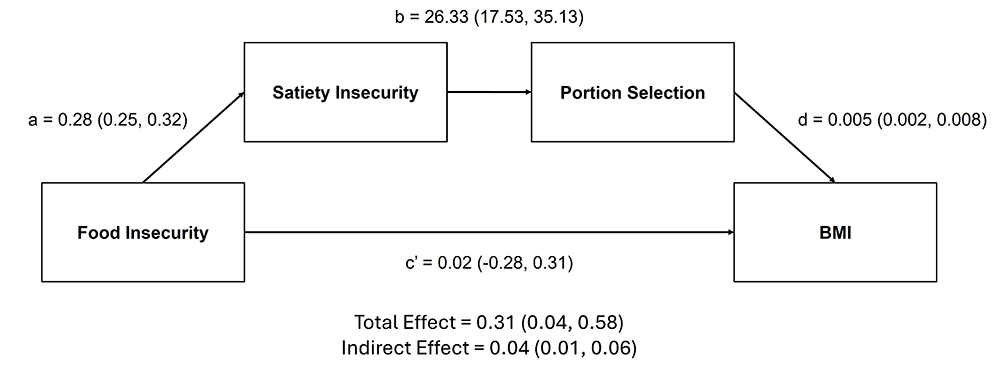
Figure 2. Serial mediation depicting indirect effects of satiety insecurity and portion selection on the relationship between food insecurity and BMI
Food insecurity is associated with higher satiety insecurity, which is associated with selection of larger virtual food portion sizes, which is in turn associated with higher BMI. The coefficients for the paths (a, b, c’, and d) and the total and indirect effects are based on aggregating individual participant data across six studies into an individual participant database meta-analysis (total n = 1,240). Coefficients are un-standardized and pooled across 25 multiply imputed datasets. Parentheses indicate 95% confidence intervals.
Additional Funding
- K99/R00 Pathway to Independence Award to Julia Bittner
- NICHD Early Career Award to Julia Bittner
Publications
- Food insecurity may promote opportunistic eating through heightened satiety insecurity. Am J Clin Nutr 2025 122:1748-1758
- Contributions of subjective status to eating behaviors, obesity, and metabolic health across development. Appetite 2025 204:107735
- Lower subjective status is associated with reduced satiation and satiety among children and adolescents: A laboratory study. Appetite 2025 122:107811
- Socioeconomic mobility, metabolic health, and diet: mediation via subjective socioeconomic status. Obesity 2024 32:2035-2044
- Lower subjective social status is associated with increased adiposity and eating in the absence of hunger among children reporting teasing distress. J Pediatr Psychol 2024 49:462-472
Collaborators
- Zhen Chen, PhD, Biostatistics and Bioinformatics Branch, NICHD, Bethesda, MD
- Ciarán Forde, PhD, Wageningen University & Research, Wageningen, The Netherlands
- Stephen Gilman, ScD, Social and Behavioral Sciences Branch, NICHD, Bethesda, MD
- Jennifer Howell, PhD, University of California Merced, Merced, CA
- Albert Lee, PhD, Nanyang Technological University, Singapore
- Tonja Nansel, PhD, Social and Behavioral Sciences Branch, NICHD, Bethesda, MD
- Aimee Pink, PhD, Agency for Science, Technology and Research (A*STAR), Singapore
- Jack Yanovski, MD, PhD, Section on Growth and Obesity, NICHD, Bethesda, MD
Contact
For more information, email bobby.cheon@nih.gov or visit https://www.nichd.nih.gov/about/org/dir/dph/officebranch/sbsb.