
Predictors of Bone Health in Adolescents and Young Adults

- Catherine M. Gordon,
MD, MS, Head, Adolescent Bone & Body Composition Laboratory - Milena Jovanovic, PhD, Staff Scientist
- Harinder Raipuria, DNP, FNP-C, Nurse Practitioner
- Devora Stein, MSN, CRNP, FNP, Nurse Practitioner
- Lealem Asrat, MHM, Patient Care Coordinator
- Salma Musaad, MD, PhD, Statistician
- Madeleine St Ville, PhD, Statistician
- Diana Benitez-Alvarado, BS, Postbaccalaureate Intramural Research Training Award Fellow
- Jay Cheeti, BS, Postbaccalaureate Intramural Research Training Award Fellow
- Alexandra Laufer, BA, Postbaccalaureate Intramural Research Training Award Fellow
A major focus of our research is to identify factors that, during adolescence, may influence skeletal health later in adulthood. We are studying how physical and emotional health are affected in adolescents and young women with premature ovarian insufficiency (POI) by examining both the clinical presentation and underlying causes of POI, including in childhood cancer survivors, and ovarian dysfunction due to autoimmune, genetic or idiopathic (unknown) etiologies. We are conducting an interventional study to characterize multiple health outcomes and to determine the optimal hormone replacement therapy for the adolescent population. Our lab is also using advanced tools to provide state-of-the-art assessments of bone density, body composition, and skeletal strength.
We are also investigating the skeletal phenotypes of rare genetic disorders, some of which resemble or meet criteria for skeletal dysplasias, including Hutchinson–Gilford progeria syndrome, Ollier disease, and Maffucci syndrome. In addition, we are studying the rare genetic condition androgen insensitivity syndrome (AIS), which results from mutations in the androgen receptor, leading to androgen resistance.
Another aspect of our research focuses on the relationship between skin pigmentation and bone mineral density/muscle strength, predominantly in adolescents. We are conducting research across a range of pediatric and adolescent populations with gynecologic conditions that are each associated with secondary bone loss. Using spectrophotometry, we are measuring skin pigmentation quantitatively and assessing muscle grip strength with a hand-held dynamometer. Body composition is being evaluated by DXA, which allows us to measure lean body mass, a surrogate of muscle mass, and to understand musculoskeletal health more comprehensively.
Hormone replacement therapy in adolescents with premature ovarian insufficiency (POI)
POI is a rare condition, characterized by absent or irregular menstrual cycles, which represents a significant cause of infertility in women with estrogen deficiency before the age of 40. The etiology of POI includes chromosomal (Turner syndrome, Fragile-X syndrome), iatrogenic (chemotherapy, radiation, or surgery), autoimmune, or idiopathic (unknown) causes. POI has a complex clinical presentation, including vasomotor symptoms, and decreased bone mineral density (BMD) leading to susceptibility to the development of early osteoporosis and increased fracture risk, infertility in women, as well as increased risk for cardiovascular, autoimmune diseases, and mood disorders. Hormone replacement therapy (HRT), which is the physiologic replacement of premenopausal levels of estrogen and progesterone, is the most common treatment option for women with POI, and has been shown to have a positive effect on bone and cardiovascular health in adults. However, there are only sparse data from controlled clinical trials in teenagers with POI. Therefore, we are conducting an interventional trial in adolescents with POI to characterize the most effective dose, regimen, and choice of preparation of HRT for this young patient group (ClinicalTrials.gov, NCT06851754). We are investigating the effects of this therapy on multiple health outcomes, including the skeletal phenotype using high-resolution peripheral quantitative computed tomography (HRpQCT), a cutting-edge imaging research tool that provides valuable data on bone microarchitecture and structure. We are also following changes in skeletal outcomes in response to HRT.
High-resolution peripheral computed tomography
High-resolution peripheral quantitative computed tomography (HRpQCT) is a non-invasive, low-dose 3D imaging method that affords assessments of volumetric bone mineral density and bone microarchitecture of peripheral skeletal sites, including the distal radius and distal tibia. HRpQCT has the ability to differentiate between cortical and trabecular compartments of the skeleton, providing information on both bone density and structural parameters. It is a research tool that has been found to improve the prediction of fracture risk in studies of primary and secondary osteoporosis, as well as of endocrine disorders and rare diseases that affect bone. Our lab is one of only 28 centers in North America that has an HRpQCT scanner. Low-dose radiation exposure, non-invasiveness, and high resolution make HRpQCT a valuable tool in bone research. In several chronic-disease models, we are examining the relationship between failure load (loss of load-carrying capacity), fracture risk, and other HRpQCT–derived outcomes.
Figure 1. High-resolution peripheral quantitative computed tomography (HRpQCT) images
Three-dimensional HRpQCT images of the distal radius after processing in an adolescent girl
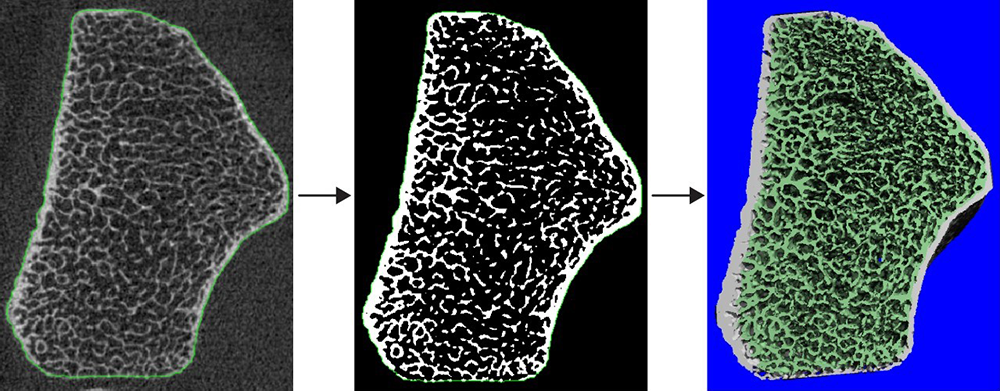
Figure 1. High-resolution peripheral quantitative computed tomography (HRpQCT) images
Three-dimensional HRpQCT images of the distal radius after processing in an adolescent girl
Evaluations of bone marrow composition
Our team is using magnetic resonance (MR) imaging and spectroscopy to evaluate bone marrow fat, which is directly influenced by hormonal signals. We studied bone marrow composition in adolescents with anorexia nervosa and are employing this technique to examine the correlation between marrow fat and bone accrual in adolescents with inflammatory bowel disease. T1 (longitudinal spin-lattice relaxation time) maps and MR spectroscopy evaluations afford a non-invasive means to evaluate bone marrow composition in children and adolescents.
Figure 2. Magnetic resonance (MR) spectroscopy assessment of bone marrow composition
MR spectroscopy images from the left knee (distal femur) of an adolescent girl with anorexia nervosa
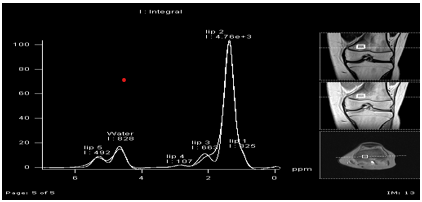
Figure 2. Magnetic resonance (MR) spectroscopy assessment of bone marrow composition
MR spectroscopy images from the left knee (distal femur) of an adolescent girl with anorexia nervosa
Additional Funding
- U01HD107957-01 (Sobreira/Gordon): Delineation of the natural history of Ollier disease and Maffucci syndrome and investigation of their genetic bases
Publications
- Impact of ovarian insufficiency on bone health in childhood cancer survivors: two cases. Bone 2024 178:116930
- Low-magnitude mechanical signals to preserve skeletal health in female adolescents with anorexia nervosa: a randomized clinical trial. JAMA Network Open 2024 7(10):e2441779
- Associations of ethnicity, skin tone, and genome-wide sequencing with bone mineral density in adolescents. Pediatr Res 2025 97(7):2376-82
- Effect of transdermal estrogen therapy on bone and neurobehavioral health in youth with premature ovarian insufficiency: a case-control study. J Pediatr Adolesc Gynecol 2025 38(4):485-491
- Lonafarnib clinical trials demonstrate uncoupling of the muscle-bone unit in Hutchinson-Gilford Progeria Syndrome. J Bone Miner Res 2025 zjaf184
Collaborators
- Leslie Bardin, MS, OTR/L, Occupational Therapy, NIH Clinical Center, Bethesda, MD
- Allessandra Brofferio, MD, Cardiovascular Branch, NHLBI, Bethesda, MD
- Tom Burklow, MD, Office of Clinical Research Training and Medical Education, NIH Clinical Center, Bethesda, MD
- Amy DiVasta, MD, MMSc, Boston Children's Hospital, Boston, MA
- Veronica Gomez-Lobo, MD, Pediatric and Adolescent Gynecology Program, NICHD, Bethesda, MD
- Rebecca Gordon, MD, Massachusetts General Hospital, Boston, MA
- Hanna Hildenbrand, MS, OTR/L, Occupational Therapy, NIH Clinical Center, Bethesda, MD
- Bonnie Hodsdon, BS, OTR/L, Occupational Therapy, NIH Clinical Center, Bethesda, MD
- Heidi Kalkwarf, PhD, RD, Cincinnati Children's Hospital Medical Center, Cincinnati, OH
- Mariana Kaplan, MD, Systemic Autoimmunity Branch, NIAMS, Bethesda, MD
- Robert Shamburek, MD, Cardio-Pulmonary Branch, NHLBI, Bethesda, MD
- Nara Sobreira, MD, PhD, Johns Hopkins School of Medicine, Baltimore, MD
- Halley Wasserman, MD, Cincinnati Children's Hospital Medical Center, Cincinnati, OH
Contact
For more information, email catherine.gordon@nih.gov or visit https://www.nichd.nih.gov/research/atNICHD/Investigators/gordon.