Physiology, Psychology, and Genetics of Obesity

- Jack A. Yanovski, MD, PhD, Head, Section on Growth and Obesity
- Joo Yun Jun, PhD, Postdoctoral Fellow
- Miranda Broadney, MD, MPH, Pediatric Endocrine Training Program Fellow
- Ovidiu Galescu, MD, Pediatric Endocrine Training Program Fellow
- Britni R. Belcher, PhD, Special Volunteer
- Nichole Kelly, PhD, Special Volunteer
- Rachel Miller-Radin, MA, Special Volunteer
- Natasha A. Schvey, PhD, Special Volunteer
- Lisa Shank, MA, Special Volunteer
- Sheila M. Brady, RN, FNP, Nurse Practitioner
- Robin Roberson, MS, Technician
- Ira S. Tigner, MS, Technical Intramural Research Training Award Fellow
- Dezmond Taylor-Douglas, BS, Graduate Student
- Nicket Dedhia, BA, Postbaccalaureate Intramural Research Training Award Fellow
- Daniel Gehle, BS, Postbaccalaureate Intramural Research Training Award Fellow
- Shannon Marwitz, BS, Postbaccalaureate Intramural Research Training Award Fellow
- Rim D. Mehari, BS, Postbaccalaureate Intramural Research Training Award Fellow
- Katherine Thompson, BA, Postbaccalaureate Intramural Research Training Award Fellow
The prevalence of overweight and obesity in children and adults has tripled during the past 40 years. The alarming rise in body weight has likely occurred because the current environment affords easy access to calorie-dense foods and requires less voluntary energy expenditure. However, such an environment leads to obesity only in those individuals whose body weight–regulatory systems are not able to control body adiposity with sufficient precision in our high calorie/low activity environment, which suggests there are subgroups in the U.S. with a uniquely high susceptibility to weight gain under the prevailing environmental conditions. Our primary goal is to elucidate the genetic underpinnings of the metabolic and behavioral endo-phenotypes that contribute to the development of obesity in children. Using our unique longitudinal cohorts of children at risk for adult obesity, who have undergone intensive metabolic and behavioral phenotyping, we examine genetic and phenotypic factors predictive of progression to adult obesity in children who are in the 'pre-obese' state, allowing characterization of phenotypes unconfounded by the impact of obesity itself. Once they are identified as linked to obesity, we study intensively genetic variants that impair gene function. We expect that these approaches will improve our ability to predict which children are at greatest risk for obesity and its comorbid conditions and will lead to more targeted, etiology-based prevention and treatment strategies for pediatric obesity.
Genetic factors important for childhood body weight regulation
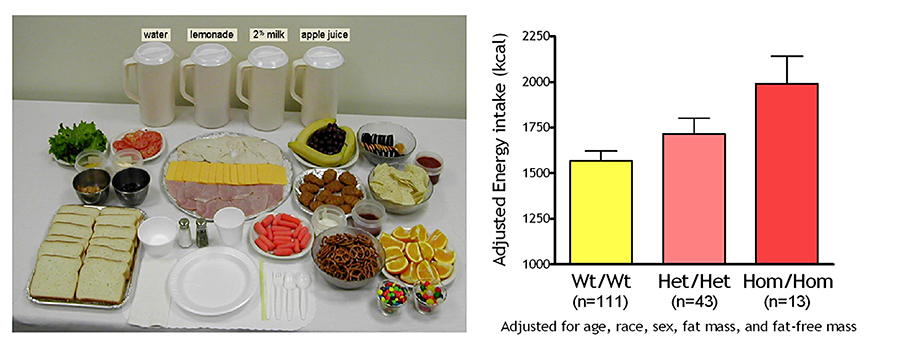
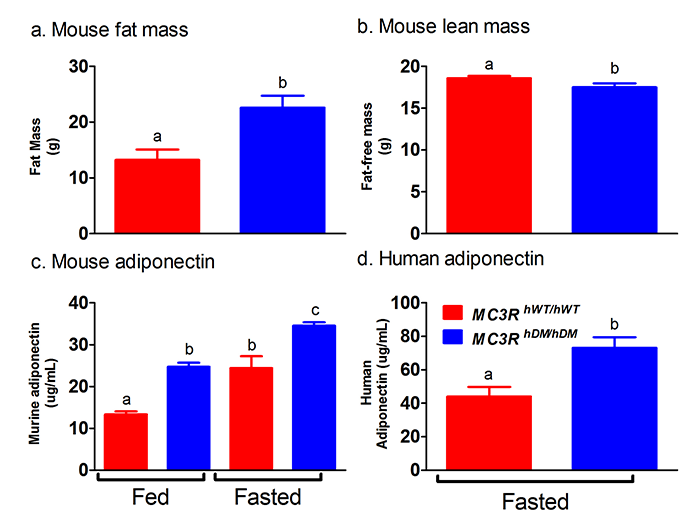
To identify gene variants affecting body composition, we have been examining polymorphisms in genes involved in the leptin signaling pathway. Genes include the leptin receptor (LEPR), FTO (fat mass and obesity-associated gene), and those encoding pro-opiomelanocortin (POMC), the melanocortin 3 receptor (MC3R), the melanocortin 4 receptor (MC4R), and brain-derived neurotrophic factor (BDNF). We are currently studying a variant MC3R that is associated with adiposity in children and appears to have functional significance for MC3R signal transduction. Children who are homozygous variant for both C17A and G241A polymorphisms have significantly greater fat mass and higher plasma levels of insulin and leptin than unaffected or heterozygous children and appear to eat more at laboratory test meals (Figure 1). In vitro studies subsequently found that signal transduction and protein expression were significantly lower for the double-mutant MC3R. Our ongoing studies attempt to understand the mechanisms by which these sequence alterations may affect body weight. We therefore developed transgenic ‘knock-in’ mice expressing the human wild-type and human double-mutant MC3R. Using homozygous knock-in mouse models replacing murine Mc3r with wild-type human (MC3RhWT/hWT) and double-mutant (C17A+G241A) human (MC3RhDM/hDM) MC3R, we found that MC3RhDM/hDM have greater weight and fat mass (Figure 2), elevated energy intake and feeding efficiency, but lower length and fat-free mass than MC3RhWT/hWT (Reference 1). MC3RhDM/hDM mice do not exhibit increased adipose tissue inflammatory cell infiltration or greater expression of inflammatory markers despite their greater fat mass. Serum adiponectin is elevated in MC3RhDM/hDM mice and MC3RhDM/hDM human subjects (Figure 2). MC3RhDM/hDM bone- and adipose tissue–derived mesenchymal stem cells (MSCs) differentiate into adipocytes that accumulate more triglyceride than MC3RhWT/hWT MSCs. MC3RhDM/hDM thus impacts nutrient partitioning to generate increased adipose tissue that appears metabolically healthy. The data confirm the importance of MC3R signaling in human metabolism and suggest a previously unrecognized role for the MC3R in adipose tissue development. Ongoing studies continue to improve our understanding of the phenotype of these mice.
Click image to enlarge.
Figure 1. Energy intake studied by using free-access buffet meals of palatable foods
Children homozygous for two polymorphisms in the MC3R gene (Hom/Hom) consumed more at the buffet than heterozygotes (Het/Het) or those with wild-type MC3R (Wt/Wt).
Click image to enlarge.
Figure 2. Studies of a human MC3R variant containing two naturally occurring polymorphisms
The variant is associated with pediatric-onset obesity. We found that mice whose Mc3r was replaced by human versions of the gene were obese when they expressed the double-mutant gene (MC3RhDM/hDM)—with greater fat mass (panel a) and lower fat-free mass (panel b), but surprisingly greater adiponectin concentrations (panel c) than mice with the normal human MC3R (MC3RhWT/hWT). Humans with the double-mutant receptor also showed greater adiponectin (panel d).
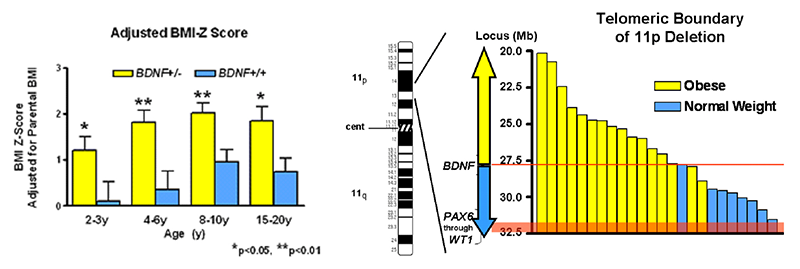
We also investigated the BDNF–TrkB pathway in relation to body mass in children. In a cohort of 328 children, aged 3–19 years, we found that obese children had significantly reduced BDNF; BMI, BMI-Z, and body fat were all negatively associated with BDNF. The data suggest that some obese individuals with low serum BDNF for age have mutations that alter BDNF function. We therefore assessed the role of BDNF haplo-insufficiency as a cause of obesity in patients with syndromes attributable to deletions in the vicinity of 11p14.1, where the human BDNF gene is located. Of 33 subjects with the WAGR (Wilms tumor, aniridia, genitourinary, and renal abnormalities) syndrome who had heterozygous 11p deletions, ranging in size from 1.0–26.5 Mb, 19 had regions of deletion that involved the BDNF gene (BDNF+/–). Compared with those with intact BDNF (BDNF+/+), BDNF+/– individuals had significantly greater body mass during childhood, starting at age two (Figure 3). A recent investigation examined common polymorphisms in the BDNF gene region. We examined human hypothalamic BDNF expression in association with 44 BDNF single-nucleotide polymorphisms (SNPs). We found that the minor C allele of rs12291063 is associated with significantly lowered human ventro-medial hypothalamic BDNF expression and greater adiposity in both adult and pediatric cohorts. We also demonstrated that the major T allele for rs12291063 binds to heterogeneous nuclear ribonucleoprotein D0B, a transcriptional regulator, knockdown of which disrupts transactivation by the T allele (Reference 2). Binding and transactivation functions are both disrupted by substitution of T with the minor C allele. The findings provide a rationale to pursue augmentation of BDNF expression and BDNF receptor signaling as targeted obesity treatments for individuals with the rs12291063 CC genotype.
Click image to enlarge.
Figure 3. WAGR syndrome and deletions of brain-derived neurotrophic factor
Patients with WAGR syndrome who have haplo-insufficiency for the brain-derived neurotrophic factor gene (BDNF) had a higher BMI standard deviation score (BMI z-score) than children and adults with WAGR syndrome who retained two copies of the BDNF gene (left panel). Deletions that extended into exon 1 of BDNF were associated with 100% risk of childhood-onset obesity (right panel).
Physiology, metabolism, and psychology of childhood body weight regulation
Our studies are directed at understanding the physiological, psychological, and metabolic factors that place children at risk for undue weight gain. As part of these studies, we examined how best to measure eating-related psychopathology, insulin sensitivity, changes in body composition, energy intake, and energy expenditure in children and we studied the short- and long-term stability of the components of the metabolic syndrome. We found that leptin is an important predictor of weight gain in children: those with high leptin levels gain more weight than children with normal leptin levels when followed longitudinally. We also documented that hyperinsulinemia is positively related to energy intake in non-diabetic, obese children, leading to treatment studies to reduce hyperinsulinemia (see below). We also examined the relationship between depressive symptomatology and insulin resistance in children and adolescents, finding strong associations both cross-sectionally and prospectively between depressive symptoms and insulin resistance independent of body weight. These associations suggest mechanisms whereby insulin resistance may contribute to excessive weight gain in children and have informed some of our treatment approaches to pediatric obesity (described below).
Our evaluations concentrating on binge-eating behaviors in children suggest that such behaviors also are associated with adiposity in children and abnormalities in metabolism. We found that binge-eating behaviors may predict future weight gain in children at risk for obesity. Children reporting binge-eating behaviors such as loss of control (LOC) over eating gained, on average, an additional 2.4 kg of weight per year compared with non-binge-eating children. Our data also suggest that children endorsing binge eating consume more energy during meals. Actual intake during buffet meals averaged 400 kcal more in children with binge eating, but, despite their greater intake, such children reported shorter-lived satiety than children without binge-eating episodes. The ability to consume large quantities of palatable foods, especially when coupled with reduced subsequent satiety, may play a role in the greater weight gain found in binge-eating children. We demonstrated that, among a cohort of 506 lean and obese youth, youth with LOC eating had significantly higher serum leptin than those without LOC episodes, even after adjusting for adiposity and other relevant covariates. The data also suggest that interventions targeting disordered eating behaviors may be useful in preventing excessive fat gain in children prone to obesity and have led to ongoing trials of preventative strategies related to binge eating. Given that binge eating appears to be a heritable trait, we also initiated studies to investigate potential genetic factors linked to LOC eating. For example, we previously reported that, among 229 youth aged 6-19 y who were genotyped for the FTO gene SNP rs9939609, subjects with at least one A allele (67.7%) had significantly greater BMI, BMI z-scores, and fat mass. We also found preliminary evidence for link between FTO SNP rs9939609 and eating in the absence of hunger.
In order to determine the factors that are most important for development of the complications of obesity in youth, we study normal-weight children and adolescents, children who are already obese, and the non-obese children of obese parents. We examine body composition, leptin concentration, metabolic rate, insulin sensitivity, glucose disposal, energy intake at buffet meals, and genetic factors believed to regulate metabolic rate and body composition. Psychological and behavioral factors, such as propensity to engage in binge-eating behavior (Figure 4), are also studied. We follow children longitudinally into adulthood. In two protocols, we study actual food consumption of children during meals, to elucidate differences in the calorie and macro-nutrient content of meals and the circulating hormones related to hunger and satiety in those who either endorse binge-eating behaviors or report no such behaviors. We found that eating in the absence of physiological hunger is a replicable trait that appears linked to obesity. We also investigated the role of sedentary behaviors, such as television watching, as a factor that alters metabolism. In a randomized, controlled, crossover trial (Figure 5), we found that glucose tolerance was markedly improved in children who engaged in moderate activity for just three minutes every half hour, versus remaining sedentary (Reference 3). We hypothesize that differences in these factors predict the development of obesity in the populations studied and may be of great importance in developing rational approaches for the prevention and treatment of obesity in the diverse US population.
Click image to enlarge.
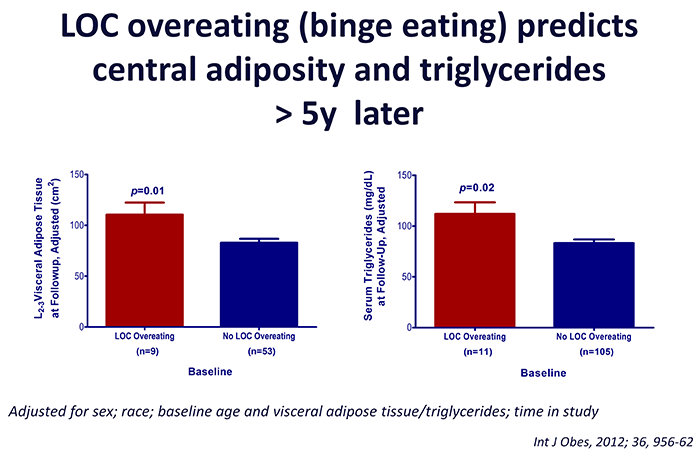
Figure 4. Loss of control (LOC) eating and metabolic complications in a longitudinal study
On average (±SE), children who engaged in binge eating at baseline had more visceral adipose tissue at L2-3 at follow-up than children who did not engage in binge eating at baseline, adjusting for sex, race, baseline age, baseline visceral adipose tissue at L2-3, and time in study (P = 0.01). On average (±SE), children who engaged in binge eating at baseline had higher follow-up triglycerides than children who did not engage in binge eating at baseline, adjusting for sex, race, baseline age, body mass index (kg/m2), baseline triglycerides, and time in study (P = 0.02).
Click image to enlarge.
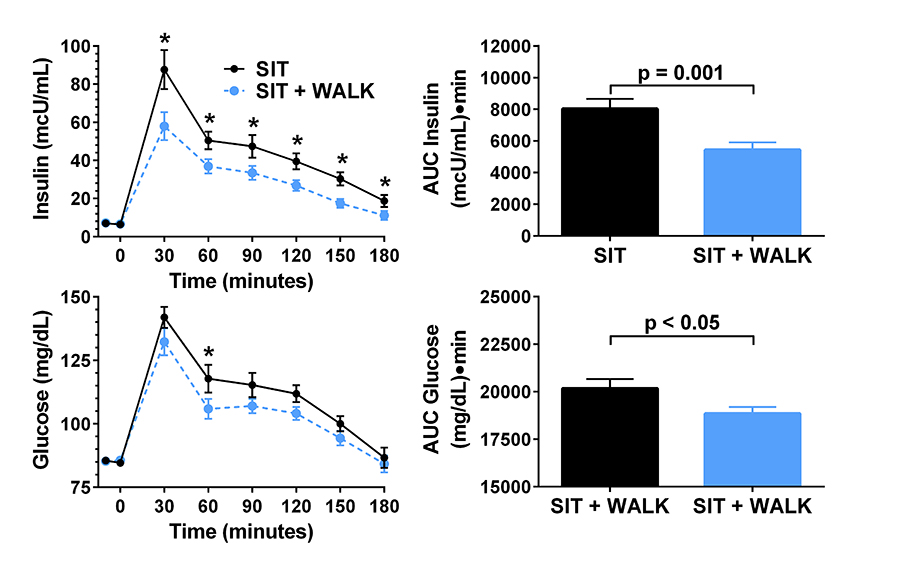
Figure 5. Effect of short, moderate intensity walking breaks on children’s glucose tolerance
Children who walked for three minutes every 30 minutes (in blue) had lower glucose and insulin concentrations during an oral glucose tolerance test than when they sat uninterrupted for three hours (in black).
Treatment of obesity and the co-morbid conditions associated with obesity
Given the rapid increase in the prevalence of obesity, the development of treatments for obesity in children and adults is urgently needed, yet current pharmacologic approaches are extremely limited for both children and adults. Thus, in several clinical protocols, we examined approaches for the prevention and treatment of excessive body weight. We completed a pilot study demonstrating that severely obese adolescents can lose weight when enrolled in a comprehensive weight management program that includes the gastrointestinal lipase inhibitor orlistat as an adjunct to a behavioral modification program. We also completed a placebo-controlled randomized trial, studying whether the weight loss of African American and Caucasian children and adolescents who have obesity-related comorbidities was improved by the use of orlistat 120 mg TID. 200 adolescents, 65% female, 61% African American, mean age 14.6 years, BMI 41.7±0.6 kg/m2 (range 27–87 kg/m2) were studied, with 85.5% of subjects completing the trial. Adolescents treated with orlistat lost significantly more weight, BMI units, and fat mass than controls. Although pulse and blood pressure fell significantly during the trial, orlistat treatment did not significantly alter these variables. Similarly, HOMA-IR (homeostasis model assessment–insulin resistance), SI (insulin sensitivity index) by FSIGT (frequently sampled intravenous glucose tolerance test), apolipoprotein B, total and LDL-cholesterol, and triglycerides fell significantly in proportion to weight loss, but orlistat use was not associated with significant reductions in any of these obesity-related laboratory comorbidities. Both liver function indicators aspartate aminotransferase (AST) and alanine aminotransferase (ALT) unexpectedly increased significantly with orlistat treatment. We concluded that orlistat added to a behavioral program significantly improved weight loss over a 6-month interval, but had little impact on obesity-related co-morbid conditions in obese adolescents.
A second obesity treatment study examined the mechanism by which metformin may affect the body weight of younger children who have hyperinsulinemia and are therefore at risk for later development of type 2 diabetes. We conducted a single-center, 6-month, randomized, double-blind, placebo-controlled trial of the effects of metformin, 1000 mg BID administered with meals, in severely obese children (6–12y) who manifested hyperinsulinemia and insulin resistance. 100 obese children (60% female, 11% Hispanic, 3% Asian, 40% African American), mean age 10.2±1.5y, with mean BMI 34.6±6.6 kg/m2 (range 23–58 kg/m2) were enrolled. 85% of subjects (84% given metformin and 86% given placebo) completed the trial. Compared with placebo-treated children, those randomized to metformin had significantly lower BMI, BMI z-scores, and body fat mass. Serum glucose and HOMA-IR also declined more in metformin-treated than in placebo-treated children. Compared with placebo, metformin treatment also elicited significant reductions from baseline in adjusted mean (+/– standard error) energy intake (metformin: –104.7 +/– 83.8 kcal vs. placebo: +144.2 +/– 96.9 kcal) independently of changes in body composition. Metformin also significantly lowered ratings of hunger and increased ratings of fullness after the pre-meal load (Reference 4). The data suggest that lower perceived hunger resulting in diminished food intake are among the mechanisms by which metformin treatment reduces body weight in overweight children with hyperinsulinemia.
A third clinical trial examined efficacy of two diets among Hispanic children and adolescents, for whom the prevalence of obesity and insulin resistance is considerably greater than in non-Hispanic white children. A low glycemic-load diet (LGD) has been proposed as an effective dietary intervention for pediatric obesity, but no published study had compared the effects of an LGD with those of a low fat diet (LFD) in obese Hispanic children. In the 113 children who were randomly assigned, the glycemic load per kilocalories of reported food intakes in participants of the LGD group was significantly lower at three months than in the LFD group. However, both groups had a significantly lower BMI z-score, which was expressed as a standard z-score relative to CDC age- and sex-specific norms, and significantly improved waist circumference and systolic blood pressure at 3, 12, and 24 months after intervention. We found no evidence that an LGD and an LFD differ in efficacy for the reduction of BMI or aspects of metabolic syndrome in obese Hispanic youth. Both diets lowered the BMI z-score when prescribed in the context of a culturally adapted, comprehensive weight-reduction program.
A fourth completed study examined prevention of weight gain using interpersonal therapy in adolescents reporting LOC eating behaviors (Reference 5). An additional study tested methods to reduce insulin resistance in adolescents at risk for type 2 diabetes. We also participated in a multi-site randomized-controlled trial of beloranib, a methionyl aminopeptidase 2 inhibitor, to treat the hyperphagia of patients with the Prader Willi syndrome. In the near future, we expect to initiate additional translational trials related to modulation of the leptin signaling pathway. Also, a novel intervention, a trial that is actively enrolling, is a randomized-controlled study of colchicine to ameliorate the inflammation that accompanies obesity and thus improve its complications.
Additional Funding
- NIH Clinical Center “Bench to Bedside” Award: Attention Bias Retraining in Adolescents with Loss of Control Eating. ORWH 2016–2017
- Office of Disease Prevention, NIH: Grant supplement to support the clinical protocol “Effects of Interrupting Sedentary Behavior on Metabolic and Cognitive Outcomes in Children.” 2016–2017
- NICHD Director's Award: “Suppression of NLRP3 Inflammasome Activation with Colchicine to Ameliorate Obesity-Associated Metabolic Abnormalities.” 2014–2016
- Zafgen Inc: “Randomized, Double-Blind, Placebo Controlled, Phase 3 Trial of ZGN-440 (Subcutaneous Beloranib in Suspension, Zafgen, Inc.) in Obese Subjects with Prader-Willi Syndrome to Evaluate Total Body Weight, Food-Related Behavior, and Safety over 6 Months.” Funds an RCT testing a new methionine aminopeptidase inhibitor in patients with Prader-Willi syndrome and obesity. 2014–2016
Publications
- Lee B, Koo J, Yun Jun J, Gavrilova O, Lee Y, Seo AY, Taylor-Douglas DC, Adler-Wailes DC, Chen F, Gardner R, Koutzoumis D, Sherafat Kazemzadeh R, Roberson RB, Yanovski JA. A mouse model for a partially inactive obesity-associated human MC3R variant. Nat Commun 2016;7:10522.
- Mou Z, Hyde TM, Lipska BK, Martinowich K, Wei P, Ong C, Hunter LA, Palaguachi GI, Morgun E, Teng R, Lai CF, Condarco TA, Demidowich AP, Krause AJ, Marshall LJ, Haack K, Voguganti S, Cole SA, Butte NF, Comuzzie AG, Nalls MA, Zonderman AB, Singleton AB, Evans MK, Martin B, Maudsley S, Tsao JW, Kleinman JE, Yanovski JA, Han JC. Human obesity associated with an intronic SNP in the brain-derived neurotrophic factor locus. Cell Rep 2015;13:1073-1080.
- Belcher BR, Berrigan D, Papachristopoulou A, Brady SM, Bernstein SB, Brychta RJ, Hattenbach JD, Tigner IL, Courville AB, Drinkard BE, Smith KP, Rosing DR, Wolters PL, Chen KY, Yanovski JA. Effects of interrupting children's sedentary behaviors with activity on metabolic function: a randomized trial. J Clin Endocrinol Metab 2015;100:3735-3743.
- Adeyemo MA, McDuffie JR, Kozlosky M, Krakoff J, Calis KA, Brady SM, Yanovski JA. Effects of metformin on energy intake and satiety in obese children. Diabetes Obes Metab 2015;17:363-370.
- Tanofsky-Kraff M, Crosby RD, Vannucci A Kozlosky M, Shomaker LB, Brady SM, Sbrocco T, Pickworth CK Stephens M, Young JF, Olsen C, Kelly NR, Radin R, Cassidy O, Wilfley DE, Reynolds JC, Yanovski JA. Effect of adapted interpersonal psychotherapy versus health education on mood and eating in the laboratory among adolescent girls with loss of control eating. Int J Eat Disord 2016;49:490-498.
Collaborators
- Silva Arslanian, MD, Children’s Hospital of Pittsburgh, Pittsburgh, PA
- Jeffrey Baron, MD, Section on Growth and Development, NICHD, Bethesda, MD
- Andrew Butler, PhD, The Scripps Research Institute, La Jolla, CA
- Nancy Butte, PhD, Baylor College of Medicine, Houston, TX
- Kong Chen, PhD, Clinical Endocrinology Branch, NIDDK, Bethesda, MD
- Anthony Comuzzie, PhD, Southwest National Primate Research Center, San Antonio, Texas
- I. Sadaf Farooqi, MD, Cambridge Institute for Medical Research, Cambridge, UK
- Oksana Gavrilova, PhD, Mouse Metabolism Core Laboratory, NIDDK, Bethesda, MD
- Joan C. Han, MD, Le Bonheur Children’s Hospital, Memphis, TN
- Steven B. Heymsfield, MD, Pennington Biomedical Research Center, Baton Rouge, LA
- Michael Jensen, MD, Mayo Clinic, Rochester, MN
- Rudolph L. Leibel, MD, Columbia University College of Physicians and Surgeons, New York, NY
- Sergey Leikin, PhD, Section on Physical Biochemistry, NICHD, Bethesda, MD
- David S. Ludwig, MD, PhD, Children’s Hospital, Boston, Boston, MA
- Cara Olsen, PhD, Uniformed Services University of the Health Sciences, Bethesda, MD
- Stephen O'Rahilly, MD, Cambridge Institute for Medical Research, Cambridge, UK
- Daniel Pine, MD, Section on Development and Affective Neuroscience, NIMH, Bethesda, MD
- Lauren B. Shomaker, PhD, University of Colorado, Boulder, CO
- Eric Stice, PhD, Oregon Research Institute, Eugene, OR
- Marian Tanofsky-Kraff, PhD, Uniformed Services University of the Health Sciences, Bethesda, MD
- B. Timothy Walsh, PhD, Columbia University College of Physicians and Surgeons, New York, NY
- Denise E. Wilfley, PhD, Washington University School of Medicine, St. Louis, MO
- Joshua Zimmerberg, MD, PhD, Section on Cellular and Membrane Biophysics, NICHD, Bethesda, MD
Contact
For more information, email yanovskj@mail.nih.gov or visit http://sgo.nichd.nih.gov.