Mechanisms of Disease in Preterm Labor and Complications of Prematurity; Prenatal Diagnosis of Congenital Anomalies

- Roberto Romero, MD, DMedSci, Chief, Program in Perinatal Research and Obstetrics
Preterm birth is the leading cause of perinatal morbidity and mortality worldwide. The Perinatology Research Branch proposed that preterm parturition is a syndrome caused by multiple pathologic processes, one of which is an untimely decline in progesterone action, manifested by "silent" shortening of the uterine cervix. Previous work conducted by our Program showed that asymptomatic women who have a cervical length less than 15mm in the second trimester of pregnancy have a 50% likelihood of delivering an early preterm neonate. However, prediction of preterm birth needs to be accompanied by a strategy to reduce the frequency of this complication. In a previous randomized clinical trial of vaginal progesterone vs. placebo in women with a short cervix, we reported that treatment was associated with a 45% reduction in the rate of preterm birth (less than 33 weeks of gestation) and a decrease in the rate of respiratory distress syndrome, the most common complication of prematurity. This year, we conducted studies to examine the relative merits of vaginal progesterone vs. cervical cerclage in patients with a short cervix and a prior history of preterm birth and found that medical treatment is as effective as the surgical approach. We also identified a novel pathologic finding associated with preterm labor without infection: chronic chorioamnionitis, which is likely attributable to maternal anti-fetal rejection, and we described a novel form of systemic fetal inflammation.
The Program also studies other great obstetrical syndromes that account for the high rate of infant mortality in the United States, including preeclampsia, fetal growth restriction, fetal death, clinical chorioamnionitis, and meconium aspiration syndrome.
Congenital anomalies continue to be a leading cause of perinatal mortality in the United States. Congenital heart disease is the leading organ-specific birth defect, as well as the leading cause of infant mortality from congenital malformations. The lack of prenatal identification of congenital heart defects can have adverse consequences for the neonate. More than half the infants affected with congenital heart disease are born to mothers without any previously known risk factors, which provides the impetus to perform a comprehensive screening examination of the fetal heart in all pregnancies. Yet, the prenatal diagnosis of congenital heart disease remains a challenge, as the sensitivity of ultrasound has ranged from 15–39%. Examination of the fetal heart is time-consuming, requiring expertise and skill. Therefore, the examination frequently does not include all the standard recommended cardiac views. Spatiotemporal image correlation (STIC) technology allows the acquisition of a volume dataset from the fetal heart and displays a cine loop of a complete single cardiac cycle in motion. A growing body of evidence suggests that 4-D sonography with STIC facilitates examination of the fetal heart. However, extracting and displaying the recommended diagnostic planes from a volume dataset that can be dissected in many ways (i.e., planes) requires an in-depth knowledge of anatomy and is difficult and operator-dependent. After several years of work, we developed a novel method for visualizing standard fetal echocardiography views from volume datasets obtained with STIC and application of "intelligent navigation" technology. We have also explored fetal brain neuroconnectivity using magnetic resonance imaging.
Development of Placenta-on-a-Chip, a novel platform to study the biology of the human placenta
NICHD launched the Human Placenta Project and affirmed that the development of new experimental methods to test placental function is a priority for the Institute and specifically called for using the "organ-on-a-chip" technology to develop a "placenta-on-a-chip".
The most important function of the placenta is the exchange of endogenous and exogenous substances, which permits an adequate supply of oxygen and nutrients, excretion of fetal metabolic waste, and protection against potentially harmful agents, such as xenobiotics, bacteria, viruses, and parasites. Prior studies on placental transport have used a wide range of experimental systems, including in vivo animal models, ex vivo placental perfusion systems, and in vitro cell cultures. In some cases, placental transfer has been studied in humans for frequently used therapeutic agents, such as antibiotics and hormones. However, such studies are difficult to perform, time-consuming, and always carry the risk of fetal exposure.
This year, we used a new bioengineering approach to model placental transport that combines micro-fluidics and micro-fabrication technologies with the culture of placenta-derived human cells to recapitulate the organ-specific architecture and physiological micro-environment critical to placental barrier function. Specifically, we developed a Placenta-on-a-Chip micro-device that enabled the compartmentalized perfusion co-culture of human trophoblasts (JEG-3) and human umbilical vein endothelial cells (HUVECs) on a thin extracellular matrix membrane (ECM) to create a physiological placental barrier in vitro. We also tested the physiological function of the micro-engineered placental barrier by measuring glucose transport across the trophoblast-endothelial interface over time. Our micro-fluidic cell culture system provided a tightly controlled fluidic environment conducive to the proliferation and maintenance of JEG-3 trophoblasts and HUVECs on the ECM scaffold. Prolonged culture in this model produced confluent cellular monolayers on the intervening membrane that together formed the placental barrier. The in vivo–like micro-architecture was also critical for creating a physiologically relevant effective barrier to glucose transport. Our Placenta-on-a-Chip model has the potential to serve as a low-cost experimental platform with a broad range of applications. This biomimetic model may also permit the quantitative analysis of placental transport of small molecules and biologics for the development and screening of new therapeutic modalities. The micro-engineering approach demonstrated in this study could also be leveraged to recapitulate key pathological features of various placental disorders to develop new types of in vitro human disease models.
Evidence of perturbations of the cytokine network in preterm labor
Click image to enlarge.
Network Medicine to Understand Preterm Labor: the Intra-amniotic Inflammatory Network in Spontaneous Preterm Labor with and without Inflammation and Infection (collaboration between the PPRO and the Section on Intercellular Interactions, Program in Physical Biology)
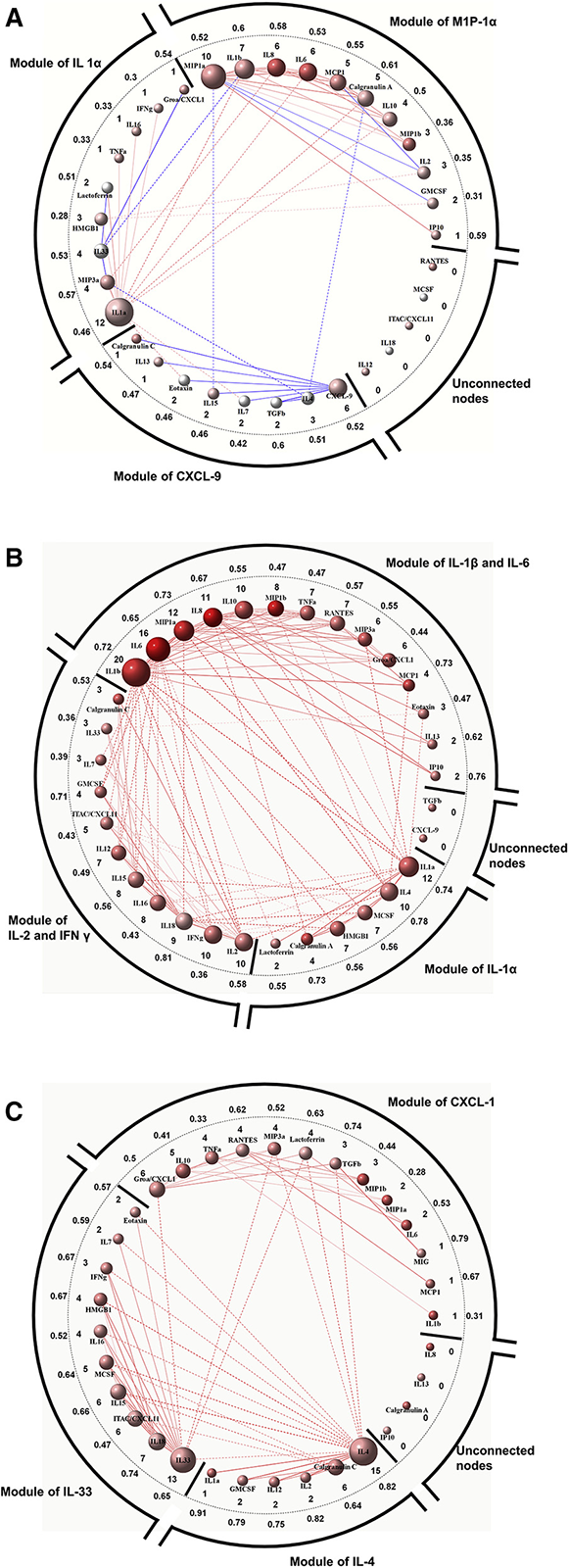
Each node (sphere) represents one of the 33 analytes, with a link (line) between two nodes that represent a significantly perturbed correlation. The node color represents the direction of concentration change (red, increased; blue, decreased; white, no change in the first group compared with the second/reference group of the comparison). The color of links gives the direction of correlation change (red, increased correlation; blue, decreased correlation); the type of line denotes the nature of the link (solid line, within module link; dashed line, cross-module link). Thick radial lines separate the modules and the set of unconnected nodes. The numbers inside/outside the dotted black circle represent the node degree/average absolute difference in correlations.
A. Network of perturbed inflammatory-related protein concentration correlations between sterile intra-amniotic inflammation and no intra-amniotic inflammation.
B. Network of perturbed inflammatory-related protein concentration correlations between microbial-associated intra-amniotic inflammation and no intra-amniotic inflammation.
C. Network of perturbed inflammatory-related protein concentration correlations between microbial-associated intra-amniotic inflammation and sterile intra-amniotic inflammation.
Intra-amniotic infection/inflammation is the only mechanism of disease with persuasive evidence of causality for spontaneous preterm labor/delivery. Previous studies on the behavior of cytokines in preterm labor were based largely on the analysis of the behavior of each protein independently. Emerging evidence indicates that the study of biologic networks can provide insight into the pathobiology of disease and improve biomarker discovery. The goal of this study was to characterize the network of inflammatory-related proteins in the amniotic fluid in patients with preterm labor.
Patients with preterm labor and intact membranes who had microbial-associated intra-amniotic inflammation had a higher amniotic fluid inflammatory-related protein concentration correlation than those without intra-amniotic inflammation (113 perturbed correlations). Interleukin-1beta (IL-1β), IL-6, macrophage inflammatory protein-1α, and IL-1α were the most connected nodes (highest degree) in this differential correlation network. Patients with sterile intra-amniotic inflammation had correlation patterns of inflammatory-related proteins that were both increased and decreased when compared with those without intra-amniotic inflammation (50 perturbed correlations). IL-1α, macrophage inflammatory protein-1α, and IL-1β were the most connected nodes in this differential correlation network. There were more coordinated inflammatory-related protein concentrations in the amniotic fluid of women with microbial-associated intra-amniotic inflammation than in those with sterile intra-amniotic inflammation (60 perturbed correlations), with IL-4 and IL-33 having the largest number of perturbed correlations (see Figure).
We reported, for the first time, an analysis of the inflammatory-related protein network in spontaneous preterm labor. Patients with preterm labor who had microbial-associated intra-amniotic inflammation had more coordinated amniotic fluid inflammatory-related proteins than either those with sterile intra-amniotic inflammation or those without intra-amniotic inflammation. The correlations were also stronger in patients with sterile intra-amniotic inflammation than in those without intra-amniotic inflammation. The findings could be of value in the development of biomarkers of preterm labor.
A point-of-care test for interleukin-6 in amniotic fluid
Preterm premature rupture of membranes (PROM) accounts for 30-40% of spontaneous deliveries at less than 37 weeks of gestation and is a major cause of perinatal morbidity and mortality. Amniotic fluid (AF) interleukin-6 (IL-6) concentrations can identify patients with intra-amniotic inflammation, at risk of impending preterm delivery and adverse pregnancy outcome. The conventional method to determine IL-6 concentrations in AF is an enzyme-linked immunosorbent assay (ELISA). However, the, technique is not available in clinical settings, and the results may take several days to become available. A lateral flow-based immunoassay, or point-of-care test, has been developed to address these challenges. We conducted a study to compare the performance of AF IL-6 determined by the point-of-care test (POCT) with that determined by ELISA for the identification of intra-amniotic inflammation and for assessing risk of spontaneous preterm delivery in patients with preterm PROM. The study included 56 women with singleton pregnancies who presented with preterm PROM. The findings were, first, a positive POCT for AF IL-6 concentrations had 97% sensitivity and 96% specificity for the identification of intra-amniotic inflammation, as defined by ELISA; and second, results of the POCT were equivalent to those determined by ELISA in identifying patients with microbial invasion of amniotic cavity, as well as those with acute inflammatory lesions of the placenta. The findings suggest that a POCT for AF concentrations of IL-6 can be used in place of ELISA to identify intra-amniotic inflammation in women with preterm PROM. Results can be available within 20 minutes, which makes it possible to quickly implement interventions designed to treat intra-amniotic inflammation and improve pregnancy outcome.
Antibiotic treatment of patients with preterm prelabor rupture of membranes
PROM affects 10% of all pregnant women, and preterm PROM occurs in 1% of all gestations. PROM in the preterm gestation accounts for 30% of all preterm births. The administration of antibiotics to patients with preterm PROM has become the standard of practice and is effective in increasing the duration of the latency period and reducing the rate of clinical chorioamnionitis and neonatal sepsis. Studies reported by our Branch provided evidence that antibiotics administration do not eradicate subclinical intra-amniotic infection in patients with preterm PROM or prevent subsequent infection. This led us to conduct a retrospective study of the outcome of pregnancy in patients given conventional antimicrobial vs. a new combination of antibiotics effective against ureaplasma species and anaerobic bacteria. We compared perinatal outcomes in 314 patients with PROM at less than 34 weeks receiving antimicrobial regimen 1 (ampicillin and/or cephalosporins; n=195) with regimen 2 (ceftriaxone, clarithromycin, and metronidazole; n=119). The outcomes of preterm PROM treated with standard antibiotic administration vs. a new combination proved that the new combination, consisting of ceftriaxone, clarithromycin, and metronidazole, prolonged the latency period, reduced acute histologic chorioamnionitis and funisitis and improved neonatal outcomes in patients with preterm PROM. The studies call for a reexamination of the current clinical practice and suggest that alternative antimicrobial agents may be more effective in this common complication of pregnancy.
Elastography to assess biophysical properties of the human cervix and the risk of preterm delivery
A sonographically identified short cervix is the most powerful predictor of spontaneous preterm birth, the leading cause of perinatal morbidity and mortality worldwide. However, only half of women with a sonographic short cervix have a preterm delivery; therefore, to avoid unnecessary treatment, there is a need to identify those women with a short cervix not at risk for preterm delivery.
Throughout gestation, the cervix undergoes dynamic changes in tissue composition characterized by dynamic remodeling of the collagen network and an increasing concentration of glycosaminoglycans and water content in the extracellular matrix, which change the biophysical properties of the organ. Elastography is a sonographic technique for estimating tissue displacement or deformation when oscillatory compression is applied. Tissue displacement or strain can be tracked, using Doppler techniques or cross-correlation analysis, and converted to an elastic modulus as an indirect estimation of tissue stiffness. We proposed that elastography examination of the uterine cervix may help identify patients with a short cervix who may be at low risk for preterm delivery.
We used quasi-static elastography to estimate cervical strain in 545 pregnant women with singleton gestations from 11 to 28 weeks of gestation. Cervical strain was evaluated in one sagittal plane, and in cross-sectional planes of both the internal cervical os and external cervical os. Women with strain values in the 3rd or 4th quartiles at the internal cervical os had a higher risk of spontaneous preterm delivery at 34 weeks or less and less than 37 weeks of gestation than women with the lowest quartile strain values. Even after adjusting for gestational age and a short cervix, women with strain values in the 3rd quartile maintained a significantly elevated risk for spontaneous preterm delivery, while those with highest quartile strain values had a marginally increased risk (compared with women with lowest quartile strain values). This is the first study describing a relationship between cervical strain and preterm delivery at 34 weeks or less and magnitudes of association between cervical strain and preterm delivery adjusted for both gestational age at examination and the presence of a short cervix. The study lays the groundwork for further investigation on the clinical benefit of elastography in combination with cervical length measurement to identify women at risk for spontaneous preterm delivery.
Biomarkers to predict induced preterm delivery
Inducted or induced preterm deliveries account for 30% of all preterm births and occur because of maternal and/or fetal indications such as preeclampsia or intrauterine growth restriction. Small-for-gestational-age (SGA) fetuses could be constitutionally small or be the result of intrauterine malnutrition. The differential diagnosis between these two conditions has been a challenge. This year, we reported a study that determined whether maternal plasma concentrations of specific biomarkers (angiogenic and anti-angiogenic factors) can predict which mothers diagnosed with suspected SGA will develop preeclampsia or require an indicated early preterm delivery (at 34 weeks of gestation or less), and whether risk assessment performance is improved using these proteins in addition to clinical factors and Doppler parameters. The study included 314 women with singleton pregnancies diagnosed with suspected SGA (estimated fetal weight less than the 10th percentile) between 24 and 34 weeks of gestation. We found that the biomarkers measured in maternal blood between 24–34 weeks of gestation can indeed identify the majority of mothers diagnosed with suspected SGA who subsequently develop preeclampsia or those who require preterm delivery at 34 weeks or less of gestation. Moreover, the addition of these biomarkers to other clinical parameters improved the prediction of preterm delivery.
Prevention of recurrent fetal death with the use of a statin
Massive perivillous fibrin deposition in the placenta and the related maternal floor infarction are serious conditions associated with recurrent complications including fetal death and severe fetal growth restriction. There is no method to evaluate the risk of adverse outcomes in subsequent pregnancies, or effective prevention. Recent observations reported by our Branch discovered that maternal floor infarction is characterized by an imbalance in angiogenic/anti-angiogenic factors in early pregnancy. Statins can increase the production of angiogenic factors and inhibit anti-angiogenic forces. We reported for the first time the use of statins to prevent recurrent fetal death. Abnormalities in the anti-angiogenic factor sVEGFR-1 and soluble endoglin were detected early in the index pregnancy, and treatment with pravastatin corrected the abnormalities. Treatment resulted in a live-birth infant near term who had normal biometric parameters and developmental milestones at the age of 2. This is the first reported successful use of pravastatin to reverse an angiogenic/anti-angiogenic imbalance and prevent fetal death. Whether other interventions can reverse the anti-angiogenic state associated with massive perivillous fibrin deposition in the placenta remains to be established.
Fetal cardiac examination using Fetal Intelligent Navigation Echocardiography (FINE)
Congenital heart disease is the most common group of malformations affecting both fetuses and newborn infants. Up to 90% of cases of cardiac defects occur in pregnancies without high risk features, which provides the impetus to perform a comprehensive screening examination of the fetal heart in all women to maximize the detection of heart defects. Yet, even when more than 90% of women in the population undergo a prenatal ultrasound examination, studies report a low sensitivity (22.5%–52.8%) in the detection of congenital heart disease, which has been attributed to issues related to operator-dependent factors. Some of the limitations of conventional two-dimensional ultrasound could be addressed by technological advances designed to reduce operator dependency. Four-dimensional sonography with spatiotemporal image correlation (STIC) allows acquisition of volume datasets of the fetal heart, and displays a cine loop of a complete single cardiac cycle in motion. Such sonographic volumes allow cardiac planes to be extracted and displayed in any orientation; however, the process requires an in-depth knowledge of anatomy and is difficult, operator-dependent, and time-consuming.
Recently, we developed and reported a novel method known as Fetal Intelligent Navigation Echocardiography (FINE), which interrogates STIC volume datasets using intelligent navigation technology. The method allows the automatic display of nine standard fetal echocardiography views required to diagnose most cardiac defects, can simplify examination of the fetal heart, and reduce operator dependency. This year, we conducted a study to prospectively evaluate the performance of the FINE method applied to STIC volume datasets of the normal fetal heart acquired between 19 and 30 weeks of gestation. One or more STIC volumes were successfully obtained in 72.5% (150/207) of women undergoing ultrasound examination. Approximately 96% (n=351) of STIC volumes evaluated by STICLoop were determined to be appropriate. Nine fetal echocardiography views were generated by the FINE method using a combination of diagnostic planes and/or VIS-Assistance® (Virtual Intelligent Sonographer Assistance) in 98–100% of cases. For each STIC volume dataset, 86% of volumes demonstrated either 8 or all 9 echocardiography views (via diagnostic planes), while 98% of volumes demonstrated all 9 echocardiography views (via VIS-Assistance®). For each STIC volume dataset, the success rate of obtaining four views (four chamber, left ventricular outflow tract, short-axis view of great vessels/right ventricular outflow tract, abdomen/stomach) was 93% and 100%, using diagnostic planes and VIS-Assistance®, respectively. The findings thus suggest that FINE could be implemented for fetal cardiac anomaly screening during routine prenatal care.
Publications
- Romero R, Grivel JC, Tarca AL, Chaemsaithong P, Xu Z, Fitzgerald W, Hassan SS, Chaiworapongsa T, Margolis L. Evidence of perturbations of the cytokine network in preterm labor. Am J Obstet Gynecol 2015; 213(6):836.e1-836.e18..
- Garcia M, Yeo L, Romero R, Haggerty D, Giardina I, Hassan SS, Chaiworapongsa T, Hernandez-Andrade E. Prospective evaluation of the fetal heart using Fetal Intelligent Navigation Echocardiography (FINE). Ultrasound Obstet Gynecol 2015; E-pub ahead of print.
- Kim CJ, Romero R, Chaemsaithong P, Kim JS. Chronic inflammation of the placenta: definition, classification, pathogenesis, and clinical significance. Am J Obstet Gynecol 2015; 213(4Supp):S53-69.
- Lee JS, Romero R, Han YM, Kim HC, Kim CJ, Hong JS, Huh D. Placenta-on-a-chip: a novel platform to study the biology of the human placenta. J Matern Fetal Neonatal Med 2015; 29(7):1046-54.
- Chaiworapongsa T, Romero R, Korzeniewski SJ, Chaemsaithong P, Hernandez-Andrade E, Segars JH, DeCherney AH, McCoy MC, Kim CJ, Yeo L, Hassan SS. Pravastatin to prevent recurrent fetal death in massive perivillous fibrin deposition of the placenta (MPFD). J Matern Fetal Neonatal Med 2015; 29(6):855-62.
Collaborators
- Tinnakorn Chaiworapongsa, MD, Wayne State University School of Medicine, Detroit, MI
- Agustin Conde-Agudelo, MD, Wayne State University School of Medicine, Detroit, MI
- Jean-Charles Grivel, PhD, Program in Physical Biology, NICHD, Bethesda, MD
- Mark Haacke, PhD, Wayne State University School of Medicine, Detroit, MI
- Sonia Hassan, MD, Wayne State University School of Medicine, Detroit, MI
- Edgar Hernandez-Andrade, MD, Wayne State University School of Medicine, Detroit, MI
- Dan Dongeun Huh, PhD, University of Pennsylvania, Philadelphia, PA
- Chong-Jai Kim, MD, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea
- Steven J. Korzeniewski, PhD, MSc, MA, Wayne State University School of Medicine, Detroit, MI
- Leonid Margolis, PhD, Program in Physical Biology, NICHD, Bethesda, MD
- Adi L. Tarca, PhD, Wayne State University, Detroit Medical Center, Detroit, MI
- Moriah Thomason, PhD, Wayne State University School of Medicine, Detroit, MI
- Lami Yeo, MD, Wayne State University School of Medicine, Detroit, MI
- Bo Hyun Yoon, MD, PhD, Seoul National University, Seoul, Korea
Contact
For more information, email romeror@mail.nih.gov or visit irp.nih.gov/pi/roberto-romero.