Pathophysiology and Genetics of Congenital Adrenal Hyperplasia

- Deborah P. Merke, MD, MS, Chief, Section on Congenital Disorders
- Ashwini Mallappa, MD, Staff Clinician
- Diala El-Maouche, MD, MS, Staff Clinician
- Qizong Lao, PhD, Staff Scientist
- Vipula Kolli, PhD, Research Fellow
- Ahmed Torky, MD, Pediatric Endocrine Training Program Fellow
- Elizabeth Joyal, MSN, Nurse Practitioner
- Padmasree Veeraraghavan, RN, BSN, Clinical Nurse Specialist
- Rahul Jayakrishnan, BA, Postbaccalaureate Fellow
- Hannah Kim, BS, Postbaccalaureate Fellow
- Kira Lokhmatova, BA, Postbaccalaureate Fellow
Congenital adrenal hyperplasia (CAH), in its most severe classic form, is a life-threatening rare orphan disease that is part of the neonatal screen performed in all 50 U.S. states. In its mildest nonclassic form, CAH is considered one of the most common autosomal recessive diseases and may be a common cause of female infertility. Our intramural NIH research program strives to elucidate the pathophysiology and genetics of CAH, leading to the development of new approaches to diagnosis, evaluation and treatment of this disease. We are conducting the largest ever Natural History Study of CAH, with over 400 patients enrolled. We were the first to identify adrenaline deficiency as a new hormonal imbalance in CAH and the first to report in CAH smaller-than-normal amygdala, the emotion regulator of the brain, providing insight into hormonal effects on the brain. We found that approximately 10 percent of patients with CAH due to 21-hydroxylase deficiency have a contiguous gene deletion syndrome resulting in CAH with a connective tissue dysplasia, Ehlers Danlos syndrome, representing a novel phenotype named CAH-X. Central to our work is the study of new treatments, including a long-term trial testing sex hormone blockade in children, and novel ways of replacing cortisol aimed at mimicking the normal circadian rhythm of cortisol secretion. The NIH Clinical Center is the ideal venue in which to carry out these studies and is one of the few places in the world that facilitates the conduct of long-term studies of rare diseases.
Identifying the phenotype and genotype of CAH-X
CAH is most commonly caused by 21-hydroxylase deficiency. The gene encoding 21-hydroxylase, CYP21A2, and a highly homologous pseudogene, CYP21A1P, are mapped to the short arm of chromosome 6 within the human leukocyte antigen histocompatibility complex. Deleterious sequence in the CYP21A1P pseudogene can be transferred to the CYP21A2 functional gene by homologous recombination, and such events produce common mutations that account for approximately 95% of all CYP21A2 disease causing mutations. Of these common mutations, approximately 30% are large deletions. The TNXB gene encoding tenascin-X, an extracellular matrix protein that is highly expressed in connective tissue, and a highly homologous pseudogene, TNXA, flank CYP21A2 and CYP21A1P, respectively. Autosomal recessive tenascin X deficiency was described as a cause of Ehlers Danlos syndrome in 2001. We hypothesized that deletions of CYP21A2 might commonly extend into the TNXB gene and have been studying this phenomena in our Natural History Study.
The first evaluation of the potential clinical implications of TNXB heterozygosity in CAH patients was performed in our Natural History Study of CAH (www.ClinicalTrials.gov Identifier no. NCT00250159) at the NIH Clinical Center. We prospectively studied 193 consecutive unrelated patients with CAH with clinical evaluations for manifestations of Ehlers Danlos syndrome and genetic evaluations for TNXB mutations. Heterozygosity for a TNXB deletion was present in 7% of CAH patients; these CAH patients were more likely than age-and sex-matched CAH patients with normal TNXB to have joint hypermobility, chronic joint pain, multiple joint dislocations and a structural cardiac valve abnormality by echocardiography (Merke DP, et al., J Clin Endocrinol Metab 2013;98:E379-387). Six of 13 probands had a cardiac abnormality including the rare finding of a quadricuspid aortic valve, a left ventricular diverticulum and an elongated anterior mitral valve leaflet. As a result of this study, the term CAH-X was coined to describe the subset of CAH patients who display an Ehlers Danlos syndrome phenotype due to the monoallelic presence of a CYP21A2 deletion extending into the TNXB gene.
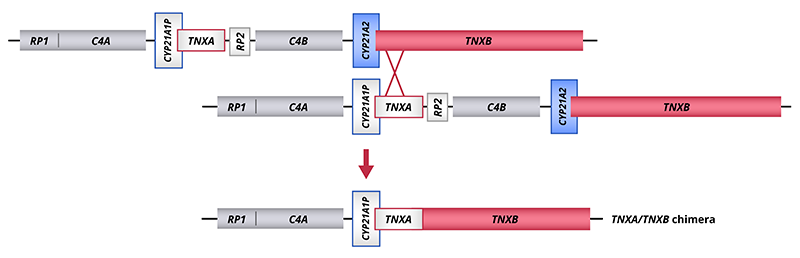
The study of CAH-X has provided insight into the recombination events that occur in the class III region of the MHC locus. This region of the genome is predisposed to genetic recombination and misalignment during meiosis. The majority of deletions that occur generate chimeric CYP21A1P/CYP21A2 genes. Similarly, chimeric recombination between TNXB and TNXA occurs (Figure). This type of recombination event deletes CYP21A2, and therefore represents a CAH disease-causing allele. We have described 3 unique types of TNXA/TNXB chimera (CH): CAH-X CH-1 retains a TNXA pseudogene derived 120-bp deletion and renders the gene nonfunctional, resulting in reduced dermal and serum TNX expression; CAH-X CH-2 deletes a cysteine that forms a disulfide bond (p.C4058W) and computational studies show that it alters protein structure; CAH-X CH-3 changes three residues (p.R4073H, p.D4172N, and p.S4175N) and the p.R4073H change is predicted to reduce protein folding energy by interfering with a cation-pi interaction between p.R4073 and p.F4080 (Reference 1). Our laboratory continues to investigate how TNXB contributes to the phenotype of CAH patients.
Click image to enlarge.
Schematic of the tenascin genes undergoing unequal crossover during meiosis resulting in formation of a TNXA/TNXB chimera.
Merke DP, et al., J Clin Endocrinol Metab 2013;98:E379-387.
To date, we have described 24 patients (19 families) with monoallelic CAH-X and 3 patients with biallelic CAH-X. Approximately 10 percent of patients with CAH due to 21-hydroxylase deficiency are now estimated to be affected by CAH-X. Overall, CAH-X patients have generalized joint hypermobility, subluxations, chronic arthralgia and about 25% have cardiac structural abnormalities. Patients with biallelic CAH-X show severe skin hyperextensibility with delayed wound healing and significant joint hypermobility (Reference 1). Other connective tissue disease manifestations in CAH-X patients include chronic tendonitis and/or bursitis, rectal prolapse, severe gastroesphagelal reflux and cardiac abnormalities.
Recessively inherited CYP21A2 point mutations or deletions cause CAH; however, TNXB mutations or deletions have autosomal dominant expression. Thus, family members of CAH patients are at risk for tenascin-X deficiency and associated connective tissue abnormalities. In general, carrying a contiguous deletion of the CYP21A2 and TNXB genes results in a more severe Ehlers Danlos syndrome phenotype in CAH patients than in their CAH unaffected relatives.
Tenascin-X is believed to serve as a scaffold for ECM organization and serves a role in elastogenesis. Although its exact mechanism of action is unknown, interactions with TGFβ have been identified. In vitro experiments using patient fibroblasts are being done to evaluate the expression of the TGFβ/BMP pathway in CAH-X patients, and the functional significance of newly identified genetic variants.
The identification of CAH-X syndrome provides insight into the complex clinical and genetic characteristics associated with CAH and promises to improve patient outcome through the development of focused medical management aimed at preventing long-term consequences.
Defining the prevalence of nonclassic CAH
The epidemiology of the classic or severe life-threatening form of CAH due to 21-hydroxylase deficiency is well established (1:10,000 to 1:20,000 live births) due to the neonatal screening of millions of newborns worldwide in over 40 countries. Neonatal screening does not accurately detect nonclassic CAH, therefore data on the prevalence of the milder form of the disorder are lacking. In a 1985 HLA-B linkage study of 210 families (43 families with nonclassic CAH), nonclassic CAH was estimated to be the most common autosomal recessive condition with carrier rates especially high in Ashkenazi Jews. In collaboration with the Johns Hopkins University School of Medicine Epidemiology-Genetics Program, we recently genotyped 200 unrelated healthy subjects of Ashkenazi Jewish descent and 200 healthy Caucasians who did not self-identify as a specific ethnicity. Nonclassic CAH carriership was similarly found in 15% (95% CI: 10.4 - 20.7) of Ashkenazi Jews and 9.5% (95% CI: 5.8 - 14.4) of Caucasians (P = 0.13), and one subject in each cohort (1 in 200 or 0.5%, 95% CI: 0.01-2.8) had a genotype consistent with being affected with nonclassic CAH (Reference 2).
As nonclassic CAH may result in infertility which is easily treated with glucocorticoid therapy and nonclassic CAH women not receiving glucocorticoid therapy might have higher miscarriage rates than those receiving treatment, our data have important implications for preconception and infertility counseling. Screening for this common and mostly undiagnosed condition in the setting of female infertility, regardless of ethnicity, would offer the opportunity for treatment.
Exploring new and improved biomarkers
The diagnosis and management of CAH has been limited by inadequate biomarkers. Multiple pitfalls have been identified in the use of 17-hydroxyprogesterone, the most commonly used biomarker, for both diagnosis and management. In newborn screening, both false positives and false negatives are common. The development of liquid chromatography-tandem mass spectrometry (LC-MS/MS) panels of adrenal steroids has expanded the repertoire of potential new and improved steroid biomarkers. Steroids synthesized with the participation of 11β-hydroxylase (11-oxygenated C19 steroids) were recently found to be abundant in patients with CAH due to 21-hydroxylase deficiency (Turcu AF et al. Eur J Endocrinol. 2016; 174(5):601-9). With our collaborators, we examined the relationship between the serum steroid metabolome of children and adults with classic 21-hydroxylase deficiency and the presence of long-term disease complications. We found that these 11-oxygenated C19 steroids are associated with having enlarged adrenal glands and testicular tumors (Reference 3). These newly described steroids may be useful in the diagnosis and management of CAH.
Developing novel treatment approaches: Circadian cortisol replacement
Humans have biological clocks with characteristic patterns of hormone secretion. Cortisol has a circadian rhythm with levels low at sleep onset, rising between 0200hr and 0400hr, peaking in the early morning, and then declining throughout the day. Existing glucocorticoid replacement is non-physiologic and this lack of diurnal rhythm may contribute to the many adverse outcomes observed in patients with adrenal insufficiency. In CAH, physiologic cortisol replacement might improve control of adrenal androgens at lower glucocorticoid doses, thus improving patient outcome. A promising treatment approach we are studying is physiologic cortisol replacement in patients with CAH.
Our group was the first to study circadian cortisol replacement in CAH patients with the use of a modified-release formulation of hydrocortisone, Chronocort® (CRADA #02800). We first studied a once-daily bedtime administration versus thrice daily conventional hydrocortisone pills in adults with classic CAH (Verma S et al. Clin Endocrinol. 2010; 72:441–447). Although this modified-release preparation resulted in serum cortisol concentrations that followed a diurnal rhythm, serum biomarkers rose late in the day higher than with conventional hydrocortisone treatment. This product was then reformulated as a multiparticulate capsule formulation for twice-daily administration. We then successfully completed a phase 2, open-label trial of 16 adults with classic CAH (Mallappa A, et al. J Clin Endocrinol Metab. 2015; 100:1137-45). Compared to various forms of conventional therapy prior to entry, 6 months of twice daily modified-release hydrocortisone yielded improve disease control throughout the day, using lower hydrocortisone dose equivalent. Successful completion of this phase 2 study carried out at the NIH Clinical Center resulted in a multi-center international phase 3, parallel arm, randomized, open-label study to determine whether this new modified-release preparation of hydrocortisone improves short-term clinical outcome (NCT#01735617). Long-term follow-up will be carried out to evaluate outcomes.
In another approach, we successfully replaced cortisol in a physiologic manner through the use of a pump usually used to deliver insulin. A programmed 24-hour infusion of hydrocortisone was delivered subcutaneously for 6 months to 8 patients with adrenal insufficiency due to 21-hydroxylase deficiency. Following 6 months of pump therapy, patients experienced significant improvement in disease control at similar or lower daily doses of glucocorticoid, and significant improvement in quality-of-life and fatigue compared to oral conventional therapy (Reference 4).
These studies provide insight into the role circadian rhythm plays in the development of the co-morbidities associated with adrenal insufficiency. Physiologic cortisol replacement represents a novel treatment approach that promises to improve treatment outcome for patients with CAH, as well as other forms of adrenal insufficiency.
Developing novel treatment approaches: Sex steroid blockade in children
As an alternative approach to the treatment of CAH, the effects of elevated androgen and estrogen could be prevented through the use of sex steroid blockade. Short-term (2 year) administration of an anti-androgen, aromatase inhibitor and reduced hydrocortisone was shown to normalize linear growth rate and bone maturation. A prospective long-term randomized parallel study to adult height of an antiandrogen (flutamide) and an aromatase inhibitor (letrozole), and reduced hydrocortisone dose vs. conventional treatment is near completion. The main outcome is adult height and data will be compared between the treatment groups. The goal of this novel treatment approach is to normalize the growth and development of children with CAH and the ultimate determination of whether or not this treatment regimen is effective in improving the growth of children with CAH is adult height. The Clinical Center is the ideal place to carry out such a long-term study of a rare disease.
Since the inception of our study of peripheral blockade of sex hormones using an antiandrogen and aromatase inhibitor, new and improved drugs that block sex steroids have been developed. Abiraterone, an irreversible inhibitor of 17α hydroxylase, a key enzyme required for testosterone synthesis, will be studied in a multicenter Phase 1/2 study in pre-pubescent children in collaboration with extramural investigators.
Additional Funding
- Cooperative Research and Development Agreement #02800 for Age-Appropriate Hydrocortisone Formulations for the Treatment of Adrenal Insufficiency including Congenital Adrenal Hyperplasia
- Cooperative Research and Development Agreement #03054 for a Phase 2 clinical trial of ATR-101 in the treatment of patients with congenital adrenal hyperplasia
- NIH U Grant: Abiraterone Acetate in Childen with Classic 21-Hydroxylase Deficiency
Publications
- Chen W, Perritt AF, Morissette R, Dreiling JL, Bohn MF, Mallappa A, Xu Z, Quezado M, Merke DP. Ehlers-Danlos Syndrome Caused by Biallelic TNXB Variants in Patients with Congenital Adrenal Hyperplasia. Hum Mutat 2016 37(9):893-897.
- Hannah-Shmouni F, Morissette R, Sinai N, Elman M, Prezant TR, Chen W, Pulver A, Merke DP. Revisiting the Prevalence of Nonclassic Congenital Adrenal Hyperplasia in U.S. Ashkenazi Jews and Caucasians. Genet Med 2017 Epub ahead of print.
- Turcu AF, Mallappa A, Elman M, Avila NA, Marko J, Rao H, Tsodikov A, Auchus R, Merke DP. 11-Oxygenated Androgens are Biomarkers of Adrenal Volume and Testicular Adrenal Rest Tumors in 21-Hydroxylase Deficiency. J Clin Endocrinol Metab 2017 102(8):2701-2710.
- Nella AA, Mallappa A, Perritt AF, Gounden V, Kumar P, Sinaii N, Daley LA, Ling A, Liu CY, Soldin SJ, Merke DP. A Phase 2 Study of Continuous Subcutaneous Hydrocortisone Infusion in Adults with Congenital Adrenal Hyperplasia. J Clin Endocrinol Metab 2016 101(12):4690-4698.
- El-Maouche D, Arlt W, Merke DP. Congenital Adrenal Hyperplasia. Lancet 2017 Epub ahead of print.
Collaborators
- Weibke Arlt, MD, Institute of Metabolism and Systems Research, University of Birmingham, Birmingham, UK
- Richard J. Auchus, MD, PhD, University of Michigan, Ann Arbor, Michigan
- Veronica Gomez-Lobo, MD, Pediatric and Adolescent Gynecology, Children's National Health System, Washington, DC
- Parag Kumar, PharmD, Clinical Pharmacokinetics Research Laboratory, NIH Clinical Center, Bethesda, Maryland
- James Marko, MD, Radiology and Imaging Sciences, NIH Clinical Center
- Corina Millo, MD, Nuclear Medicine Department, NIH Clinical Center, Bethesda, Maryland
- Aikaterini A. Nella, MD, Division of Pediatric Endocrinology, University of Texas Medical Branch, Galveston, Texas
- Ann E. Pulver, ScD, Johns Hopkins School of Medicine, Baltimore, Maryland
- Martha Quezado, MD, Laboratory of Pathology, National Cancer Instititue, Bethesda, MD
- Richard J. Ross, MD, Academic Unit of Diabetes, Endocrinology and Reproduction, University of Sheffield, Sheffield, UK
- Ninet Sinaii, PhD, MPH, Biostatistics and Clinical Epidemiology Service, NIH Clinical Center, Bethesda, Maryland
- Steve J. Soldin, PhD, Department of Laboratory Medicine, NIH Clinical Center, Bethesda, Maryland
- Adina Turcu, MD, University of Michigan, Ann Arbor, Michigan
Contact
For more information, email dmerke@nih.gov or visit https://irp.nih.gov/pi/deborah-merke.